What If The Online Course You're Building Is Making Your Clients Worse?
Health and well-being professionals are educators long before they ever think of themselves that way. Every session, every programme, every conversation is teaching, helping someone understand, reframe, practise, and change.
But here's the uncomfortable truth the course-creation industry rarely mentions: a badly designed online course doesn't just fail to help. In health and well-being contexts, it can actively work against the people it was built to support.
This article is about what happens when we get it right and what the evidence says it takes to get there.
Why the Stakes Are Higher in Health Education
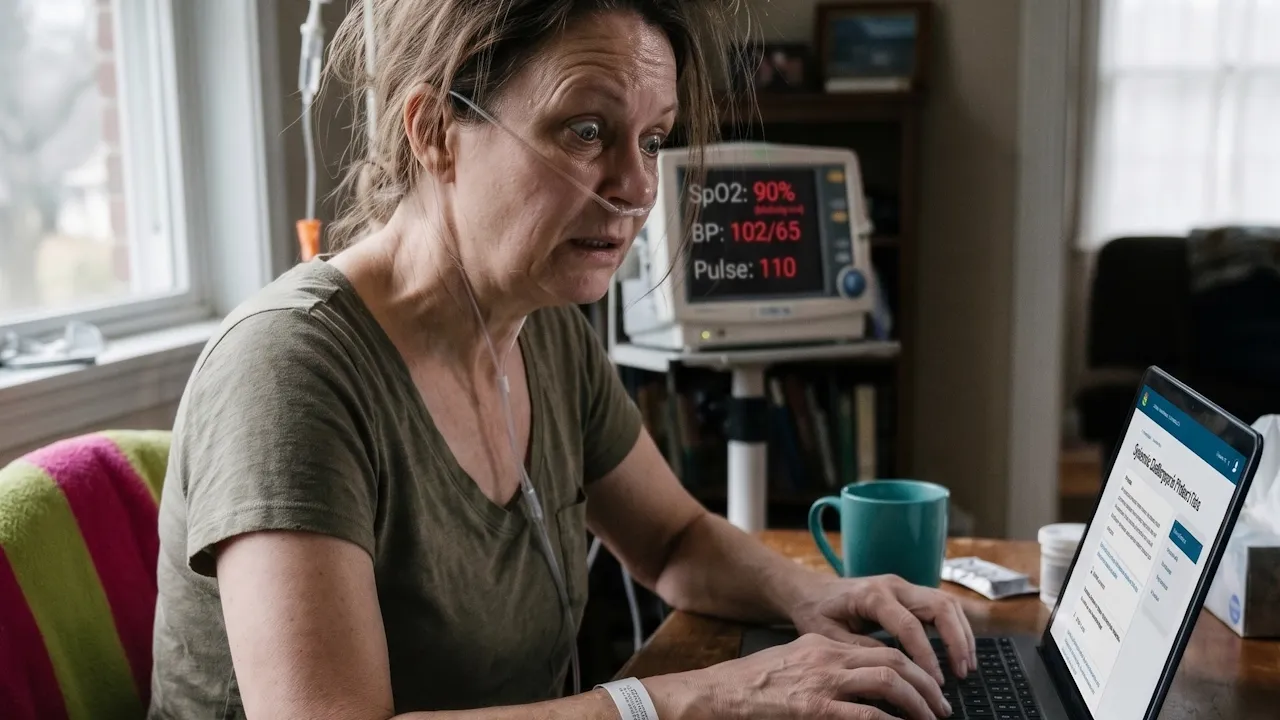
When someone signs up for a course on, say, managing anxiety, recovering from burnout, improving their relationship with food, or navigating a chronic condition, they're not doing it casually. They're doing it because something in their life needs to change.
That matters. Because learning under stress looks very different to learning out of curiosity.
|
This is the problem with so many online health and well-being courses. They're built like knowledge libraries, comprehensive, well-intentioned, and cognitively punishing.
They confuse thoroughness with support.
The Cognitive Load Problem Nobody Talks About
Cognitive load theory, first proposed by educational psychologist John Sweller in 1988, and extensively tested since, tells us that the human brain has a limited working memory. When we overload it, learning doesn't just slow down. It stops.
|
In practice, this means:
- A module with six subtopics is harder to retain than one with two
- A lesson that requires the learner to navigate three platforms is exhausting before it's even begun
- An interface with too many options creates decision fatigue, not empowerment
One practitioner we worked with described the turning point in redesigning her programme:
"Once we stripped it back to what someone actually needed to do differently — not just understand — the whole course became lighter. Clients started finishing it. Before, they just… stopped."
Structure Is Not Rigidity. It's Reassurance.
There's a persistent myth in wellness spaces that structure feels clinical, cold, or corporate. In learning design, the opposite is true.
Structure is what allows a learner to relax. When someone knows what's coming next, how long a module takes, and what they're expected to do with what they've learned, they can actually focus on learning it.
|
The 2019 systematic review in the Journal of Medical Internet Research (Beatty et al.) reinforced this, finding that well-structured digital health interventions produced significantly stronger results for behaviour change than information-dense, unstructured approaches.
This translates directly into how courses should be built:
- Lessons that are 5–12 minutes long (not 45-minute lectures)
- Predictable module layouts so learners know where to look
- Reflection prompts that invite application, not just comprehension
- Clear 'what to do next' guidance at the end of every section
"It finally feels like my work exists outside the room — without losing its integrity."
— A client on the completion of their course build
The Behaviour Change Piece Everyone Skips
Most health professionals know their subject deeply. Fewer have been trained in how humans actually change behaviour — which is the thing online courses are ultimately trying to support.
|
Self-Determination Theory (Deci & Ryan, 1985) adds another layer: people sustain behaviour change when three psychological needs are met — autonomy (they chose this), competence (they can do this), and relatedness (they're not alone in this).
Course design that serves health outcomes needs to embed all three — not as a nice extra, but as structural features.
That means:
- Offering learner choice within the course structure
- Building in early wins so people feel capable quickly
- Using language that normalises struggle rather than implying everyone else finds this easy
The Platform Is the Last Thing You Should Think About
We use Kajabi. We've used it for over 16 years. We recommend it unreservedly for health and wellbeing professionals who want a single, stable environment for their courses, community, and client communications.
But here's what we tell every practitioner we work with: the platform doesn't solve the design problem. It delivers the solution you've already built.
If the thinking is solid, if the outcomes are clear, the structure is considered, the language is human, the platform amplifies that. If the thinking is muddled, the platform scales the confusion.
One course creator we supported said, after launch:
"The difference wasn't the content. It was that learners stopped emailing me asking, 'how do I find…?' Everything finally made sense to them."
What Ethical Online Learning Looks Like
We use the word 'ethical' deliberately. In health and wellbeing contexts, the duty of care extends beyond the therapy room or consulting space. If your course reaches someone at a vulnerable moment, the design choices you make matter.
Ethical online learning in health and wellbeing:
- Does not use urgency or fear to drive engagement
- Does not promise transformation it cannot guarantee
- Respects that learners have limited time, attention, and energy
- Is honest about what a course can and cannot do
- Designs for completion, not just purchase
The most important question isn't 'Will people buy this?'
It's: Would this genuinely support someone if they found it at exactly the right moment?
When the answer is yes, the course stops being a product. It becomes part of someone's support system.
Further Reading & Sources
Schwabe, L. & Wolf, O. T. (2012). Stress effects on memory encoding: A cognitive neuroscience perspective. Frontiers in Human Neuroscience. Read here
Paas, F., Renkl, A. & Sweller, J. (2003). Cognitive Load Theory and Instructional Design: Recent Developments. Educational Psychologist, 38(1). Read here
Beatty, L. et al. (2019). Digital mental health interventions for depression, anxiety, and enhancement of psychological well-being. Journal of Medical Internet Research. Read here
World Health Organisation (2019). WHO guideline: recommendations on digital interventions for health system strengthening. Read here
Deci, E. L. & Ryan, R. M. (1985). Intrinsic Motivation and Self-Determination in Human Behaviour. Springer.
Prochaska, J. O. & DiClemente, C. C. (1983). Stages and processes of self-change of smoking. Journal of Consulting and Clinical Psychology, 51(3).
Work With Us
At The Customer's Shoes, we work with health and wellbeing professionals who want their digital offerings to feel ethical, professional, and grounded in real change.
We design courses that respect emotional and cognitive load, turn clinical expertise into structured learning journeys, and build on Kajabi all the way through to launch.
If that sounds like what you need, book a complimentary discovery call here.
Schedule a Free Discovery Call
Are you looking for support in planning, designing, creating, publishing or promoting your online courses? Schedule a call and let's explore how we can help you.
GET KAJABI FREE FOR 30 DAYS
Try Kajabi for 30 days for free.
Stay connected with news and updates!


Get Kajabi Services
We’re Certified Kajabi Experts with 16 years of hands-on Kajabi experience and 25 years of instructional design expertise, combining platform mastery with powerful learning strategies to build online course businesses that truly thrive.
From big-picture growth strategy to fully “Done-For-You” implementation, we manage every detail with precision—so you can stay focused on serving your audience. We don’t just build courses; we design transformative learning experiences that convert, engage, and retain.
Our mission is simple: unlock the full potential of your Kajabi account, maximise your ROI, and create programs your students love, and keep coming back for.


50% Complete
Add Your Details
Add your details and we will email you helpful advice and insights. You can unsubscribe at any time.